By Andy Weissberg
In the increasingly competitive, transparent and value-based healthcare economy, hospitals and health systems in Western PA and throughout the nation are facing increasing financial pressure from healthcare purchasers and payers to improve patient care outcomes. At the center of value-based purchasing and reimbursement, performance against numerous measures of quality and patient safety performance also heighten hospital concerns for reputation and market share.
Although patient safety and quality have traditionally been regarded as disparate domains of performance measurement in traditional fee-for-service (FFS) models, they are increasingly interconnected in performance-driven, value-based purchasing, payments and reimbursement from both public and private payers, underpinning the business case to improve the quality and safety of health care.
The top and bottom line: only high-performing hospitals that deliver higher quality, safer and more efficient care with measurable and improved clinical outcomes will thrive and financially survive, improving a health system’s reputation and ability to increase market share and encourage patients to use in-network services.
Measuring What Matters in Value-based Reimbursement
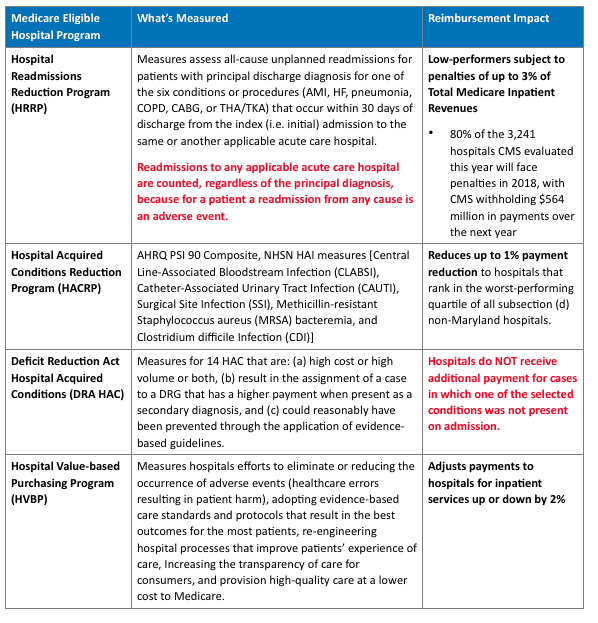
Pursuant to newly introduced regulations elaborated in the updated FY 2018 Medicare Inpatient Prospective Payment System (IPPS) Final rule, a variety of patient safety performance measures traverse several mandatory and/or voluntary value-based payment and reimbursement programs which individually, variably and collectively incentivize, penalize or withhold payments to acute care hospitals and health systems for numerous types of preventable adverse events and complications of care.
Measuring What Matters in Bundled Payment Models
Bundled payment and population management models invoke incentives for self-policing by provider organizations that must coordinate aggregate sets of clinical care, rather than episodic treatment and billing à la carte.
There are both all-inclusive prospective payment and fee-for-service models, but essentially, providers that utilize less costly services for the episode can receive a share of CMS gains; those that use costlier services for the same episode are “penalized.” In practice, the penalty scenario will be either a single prospective payment less than the sum of fee-for-service payments or a reconciliation adjustment that takes back from fee-for-service payments for the condition episode. Within a condition, there is variance in target price for co-morbidity and clinical complications involved in the episode. In addition to hitting cost targets, care must be effective—the provider must meet quality metrics to achieve a gain share. To successfully measure clinical and financial performance in bundled payments, hospitals must examine claims from various hospital departments, specialists, skilled nursing facilities, and other providers to determine their total “cost” of each episode in order to compare it with CMS’s target price.
The Centers for Medicare & Medicaid Services (CMS) announced on Tuesday, August 15, a proposed rule that reduces the number of mandatory geographic areas participating in the Comprehensive Care for Joint Replacement (CJR) Program which tests bundled payment and quality measurement for an episode of care associated with hip and knee replacements. Pursuant to the proposed rule, the number of mandatory geographic areas participating in the CJR model would drop by almost half, from 67 to 34; The Harrisburg-Carlisle, PA metropolitan service area (MSA) remains as one of the 34 geographic areas for the CJR Program.
Maximizing Reimbursement in Value-based Care Begins with Performance Management
By finding the real causes of medical errors and determining the issues, it is possible to measure safety and quality, and ultimately provide safe, quality healthcare to the patients in a way that is financially viable and legally compliant in today’s complex healthcare environment. Western Pennsylvania hospitals and health systems have greater financial motivations than ever before to adopt enterprise performance management solutions that provide a line of sight into risk-adjusted measures of quality and patient safety linked to value-based payments and reimbursement across the public and private payer mix.
Andy Weissberg is Senior Vice President of Marketing Communications for Quantros.






