
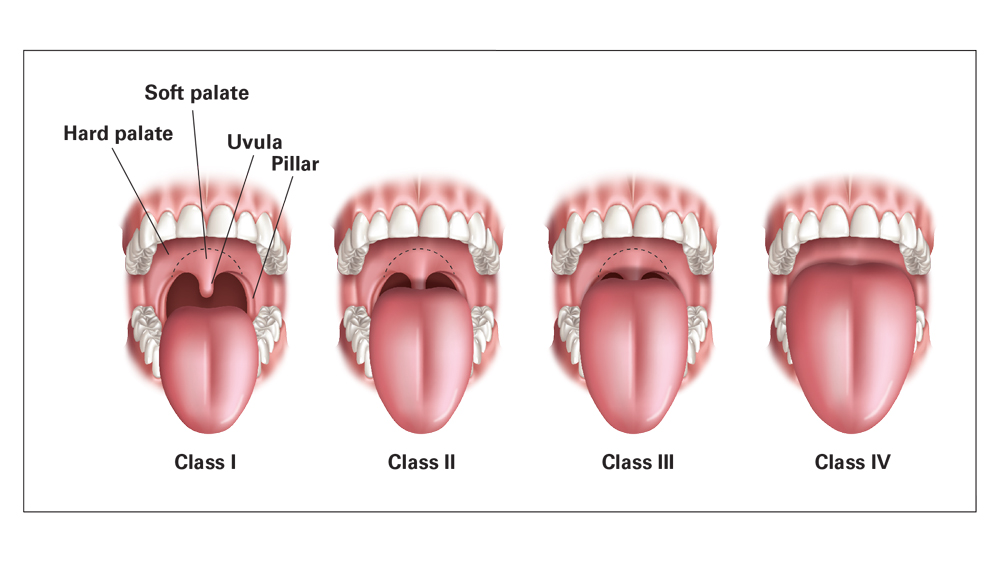
Most situations of sleep apnea are reflective of an oral obstruction to airflow and breathing. OSA (obstructive sleep apnea) is usually caused by the position of the tongue, classified as a Class IV tongue, which blocks the back of the throat, preventing air from getting in.
There may also be a narrow trachea (windpipe) due to skeletal growth failing to occur appropriately, thus creating a small house (mouth) with large furniture (tongue) blocking the airway.
Speaking of children and sleep apnea from very early development some children have mouth breathing issues.
There may also be a narrow trachea (windpipe) due to skeletal growth failing to occur appropriately, thus creating a small house (mouth) with large furniture (tongue) blocking the airway.
Speaking of children and sleep apnea from very early development some children have mouth
breathing issues.
These kids are at considerable risk for developing:
1. A narrow maxillary arch -the upper portion of your mouth that closes with your lower jaw. Limited arch space leads to teeth crowding and lack of room for your tongue. Speech development issues arise also.
2. A restricted nasal passage-the mucosa in the nose is narrow from incomplete development, causing reduced airflow as if you’re trying to breathe through a straw.
3. Obstructive sleep apnea– OSA is categorized as a disorder of breathing due to anatomic and skeletal tissue conditions that arise during the developmental phase, which minimize or reduce the necessary airflow required by the body for normal respiration.
4. Snoring- occurs as excessive, inflamed tissue in the mouth and throat vibrate as air tries to enter or exit
5. Bedwetting– due to blowing off CO2 (Carbon Dioxide)
6. Signs of poor concentration-often results because the brain can’t get rid of the waste metabolites during the deep states of rem sleep which this would typically occur in
7. Sleepiness and behavior problems at school– once again related to the disturbed sleep, which occurs with OSA.
8. Attention deficits-disorder or ADHD is a result of OSA. Family physicians are often too quick to prescribe medications to our kids without first exploring the concept of OSA.
9. Delayed development-can occur when the brain is cloudy with waste products circulating in the cerebral fluid of the brain.
10. Retrognathia (abnormal posterior positioning of the mandible)-can arise during the developmental stages of skeleton growth when the tongue is unable to serve its natural function during swallowing. Especially infant stages when breastfeeding is not done, and the infant is fed through baby bottles.
11. Adult breathing disorders-OSA as a child quickly translates later in the adult suffering from these same issues expanding and causing systemic organ problems.
12. The malocclusions-the way your teeth fit together when you close your jaw. When the teeth are not aligned correctly, the jaw cannot close quickly, this is a malocclusion.
13. Hypertension-Is when your blood pressure rises due to stresses on the body from not breathing correctly.
14. Cardiac arrhythmias– can occur when the body attempts to overcompensate from a lack of normal breathing in OSA patients.
DON’T WORRY
Sleep apnea is a treatable condition.
I frequently design sleep apnea appliances for my patients that move the lower jaw forward and prevent it from falling back during sleep, increasing the airflow. These appliances often reduce or eliminate snoring also. The patients can breathe more easily and thus reverse or prevent a number of the problems mentioned above. The TAPP appliance pictured below is very effective in the treatment of OSA.

For more information visit Greenville Dentist Dr. Leor Lindner
Author- Leor Lindner D.M.D.
Dr. Lindner graduated from Fairleigh Dickinson University in 1986 and Fairleigh Dickinson College of Dental Medicine in 1990. He completed a 1 year fellowship in TMJ-Facial pain diagnosis, treatment and management at University of Medicine and Dentistry of New Jersey.

Email- [email protected]

Dr. Lindner graduated from Fairleigh Dickinson University in 1986 and Fairleigh Dickinson College of Dental Medicine in 1990. He completed a 1 year fellowship in TMJ-Facial pain diagnosis, treatment and management at University of Medicine and Dentistry of New Jersey.






